 English
English Italiano
ItalianoAcromegaly is a syndrome that results when the anterior pituitary gland produces excess growth hormone (GH) due to a pituitary adenoma (a tumor of the pituitary gland).
Acromegaly most commonly affects adults in middle age, and can result in severe disfigurement, complicating conditions, and premature death if unchecked.
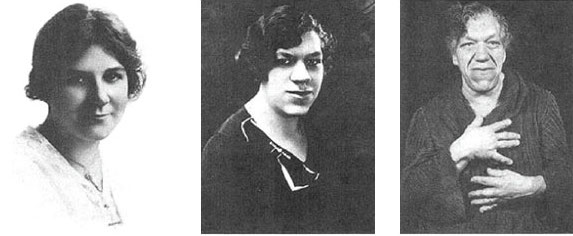
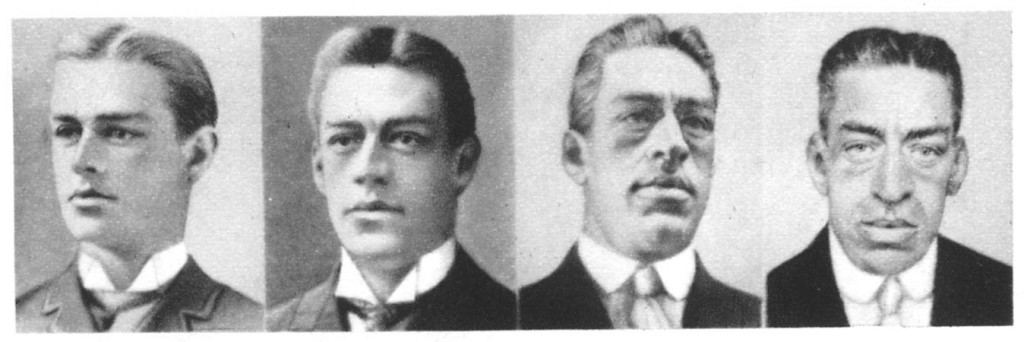
Because of its pathogenesis and slow progression, the disease is hard to diagnose in the early stages and is frequently missed for years until changes in external features, especially of the face, become noticeable.
SIGNS AND SYMPTOMS
Features that result from high level of GH or expanding tumor include:
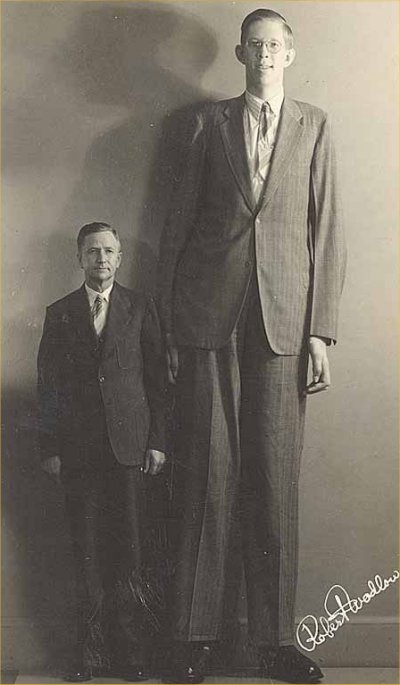
- Abnormal enlargement of the hands and feet
- Changes in facial features, sometimes quite prominent, including:
- Enlargement of forehead and jaw, widening the spaces between teeth and enlarging tongue
- Soft tissue swelling visibly resulting in enlargement of the hands, feet, nose, lips and ears, and a general thickening of the skin.
- Deepening of the voice in males
- Oily skin and excessive sweating
- Carpal tunnel syndrome
- Sleep apnea
- Arthritis
- Headache

Acromegaly: Symptoms Related to Large Tumor Size (Macroadenomas)
Macroadenomas that grow upward into the brain cavity can compress the optic chiasm. Vision problems can include:
- A loss of the outer peripheral vision, called a bitemporal hemianopsia
- When severe, a patient can only see what is directly in front of them
- Many patients do not become aware of their visual loss until it is quite severe.
Other visual problems can include:
- Loss of visual acuity (blurry vision), especially if the macroadenoma grows forward and compresses an optic nerve
- Colors not perceived as bright as usual
DIAGNOSIS
If acromegaly is suspected, medical imaging and medical laboratory investigations are generally used together to confirm or rule out the presence of this condition.
Hormone Testing
Doctors will order blood tests, specifically looking for an elevated level of IGF-1. In some rare cases, usually in premenopausal women, the GH levels can be high even though the IGF-1 levels are normal. This is an estrogen-resistant phenomenon.
Normally, the pituitary glands secrete GH in a pulsatile fashion, meaning the level increases and decreases significantly throughout the day. This affects diagnosis in two ways:
- It is difficult to diagnose acromegaly based on a random GH measurement, because a measurement at one time differs drastically from one taken at a different time.
- GH release also falls dramatically after eating a large quantity of sugar, whereas tumor cells do not exhibit this characteristic. This expected drop in hormone production is useful in helping diagnose acromegaly.
IGF-1 is released in a more steady fashion. Its levels do not go up and down quickly, making it a better hormone to measure to screen for acromegaly.
You may be asked to undergo an oral glucose tolerance test (OGTT) to confirm the diagnosis. Drinking 75 grams of a glucose solution should lower the GH level to lower than one nanogram per milliliter. In acromegalics, this suppression does not occur and may in fact increase.
Magnetic Resonance Imaging (MRI)
Magnetic resonance imaging (MRI) scan of the pituitary gland is useful to make a diagnosis.
Smaller tumors may not be visible using Computed Tomography (CT) scans.
The vast majority (90%) of GH-secreting tumors are macroadenomas.
TREATMENT
The optimal treatment of acromegaly depends on multiple factors, including:
- Size and location of the tumor
- Age and medical condition of the patient
Treatment options include:
- Surgery
- Medication
- Radiation therapy
Surgery
If the pituitary adenomas require surgery, typically the best procedure is through a nasal approach. with the minimally invasive endoscopic endonasal technique.
This procedure removes the tumor while minimizing complications, hospital time and discomfort. This advanced technique requires specialized training and equipment.
Very large tumors that extend into the brain cavity may require opening the skull (craniotomy) to access the tumor.
Medication
In some cases, doctors use medication, and not surgery, as the first course of treatment. However, in many cases, patients require both medical and surgical therapies to control acromegaly.
Medications include:
- Somatostatin analog (Octreotide, Lanreotide) injections, typically administered to patients on a monthly basis, suppress growth hormone production in about 70 percent of patients.
- Significant tumor shrinkage occurs in 30 to 50 percent of patients.
- Injections often improve symptoms of soft tissue swelling, headache, joint pains and sleep apnea.
- Patients require lifelong treatment with somatostatin.
- Drugs that block the action of growth hormone on liver cells, such as a daily injection of Pegvisomant. When effective, IGF-1 levels can normalize, but elevated growth hormones remain.
- Drugs that mimic the effect of dopamine, such as cabergoline, are effective in a small number of patients. These medications are the same ones used to treat prolactinomas.
Radiation Therapy
For some patients, surgery or medication is not sufficient to control the acromegaly. In these cases, doctors may recommend Stereotactic Radiosurgery trough highly focused dose of radiation to the tumor.
The radiation beam is designed to target only the tumor. The surrounding brain structures receive only a fraction of the radiation dose and are typically unharmed, with the exception of the normal pituitary gland.
Non-Functioning Pituitary Adenomas Cushing Disease Prolactinomas TSH-oma