English
English Italiano
ItalianoThe vertebral column (backbone) is made up of 33 vertebrae separated by spongy disks and classified into four distinct areas.
- the cervical area consists of seven bony parts in the neck
- the thoracic spine consists of 12 bony parts in the back area
- the lumbar spine consists of five bony segments in the lower back area; five sacral bones (fused into one bone, the sacrum); and four coccygeal bones (fused into one bone, the coccyx)
Between each vertebra is a fibrous disc with a jelly-like core. These cushions of cartilage allow the body to accept and dissipate load across multiple levels in the spine and still allow for the flexibility required for performing normal activities of daily living. As the body twists, bends, flexes and extends, the intervertebral discs are constantly changing their shape.
Causes
When discs degenerate, becoming less supple due to age or back strain, the disc may prolapse — squeezing out some of the soft core. This loss of cushioning may cause pressure on local nerves and cause
- back or neck pain
- numbness or tingling in the arms
- searing pain down one or both legs
If the prolapse is severe it can damage the spinal cord. As a part of the aging process the discs lose their high water content and their ability to cushion the vertebrae. This is called degenerative disc disease.
As the discs deteriorate, the spine can initially become less stable. Bony spurs can develop as a result of this instability and can cause pressure on nearby nerves leading to leg or arm pain. Narrowing of the neural canal by these bony spurs is known as degenerative spinal stenosis.
By the age of 35, approximately 30% of people will show evidence of disc degeneration at one or more levels. By the age of 60, greater than 90% of people will show evidence of disc degeneration at one or more levels on MRI. In some patients, this disc degeneration can be nearly asymptomatic; in others, disc degeneration can lead to intractable back pain.
The outer layer of the discs themselves can also tear. When this occurs, the inner, gelatinous layer can herniate out (a “herniated” or “ruptured” disc) and also cause pressure on an adjacent nerve.
If the herniation occurs in the neck and causes pressure there, it can cause pain that radiates into the shoulder and arm; if it occurs in the lower back, the pain produced can radiate down into the hip and leg.
Symptoms
Patients with disc disease in the cervical, thoracic, or lumbar spine experience variable symptoms depending on where the disc has herniated and what nerve root it is pushing on. The following are the most common symptoms of lumbar disc disease:
• Intermittent or continuous back pain
• Spasm of the back muscles
• Sciatica — pain that starts near the back or buttock and travels down the leg to the calf or into the foot.
• Muscle weakness in the legs
• Numbness in the leg or foot
• Decreased reflexes at the knee or ankle
• Changes in bladder or bowel function
In rare cases, patients with large disc herniations may experience weakness in an extremity or signs of spinal cord compression such as difficulty with gait, incoordination, or loss of bowel/bladder control.
Diagnosis
• Spine x-rays are commonly taken after a neck injury in order to rule out a fracture, dislocation or instability. Cervical spine x-rays may reveal congenital narrowing of the cervical spinal canal when present. Thoracic and lumbar x-rays may also show evidence of degenerative disease such as bone spurs and disc space narrowing.
• CT scan of the spine is valuable in assessing bone injury, such as fracture and/or dislocation. CT scan is most useful in showing bone structures, and is not as good as MRI in showing spinal cord, nerve roots or discs. CT scan does not show torn ligaments or minor tears of discs.
• MR scanning (MRI) of the spine is the best method of imaging the spinal cord and nerve roots, the intervertebral discs, and the ligaments. However, MRI findings can only be of value when they are interpreted together with and in the light of the entire clinical picture, and exactly match the clinical findings.
• Cervical myelography consists of x-rays taken after the injection of radio-opaque contrast material into the spinal fluid via a lumbar puncture, and is followed by post-myelogram CT scan of the spine (myelo-CT). It may provide useful images of the interior of the spinal canal, and can reveal indentations of the spinal fluid sac caused by bulging or herniated discs or bone spurs that might be pressing on the spinal cord or nerves. MRI provides superior images of the spinal cord, nerve roots and discs.
• Electrodiagnostic studies (EMG and nerve-conduction velocities) are useful in evaluating weakness of hand and arm or leg muscles, and can indicate whether the weakness is due to abnormality or compression of a nerve root, or to some other cause.
Treatment
Treatment for disc disorders must be closely tailored to the patient, based on:
• The history and severity of their pain
• Whether or not they have had prior treatments for this problem and how effective they have been
• Whether or not there is any evidence of neurologic damage such as weakness of an extremity or the loss of reflexes
Some of the treatments used include
• Activity modification
• Patient education on proper body mechanics (to help decrease the chance of worsening pain or damage to the disc)
• Physical therapy, which may include ultrasound, massage, conditioning, and exercise programs. Weight control
• Medications (to control pain and/or to relax muscles)
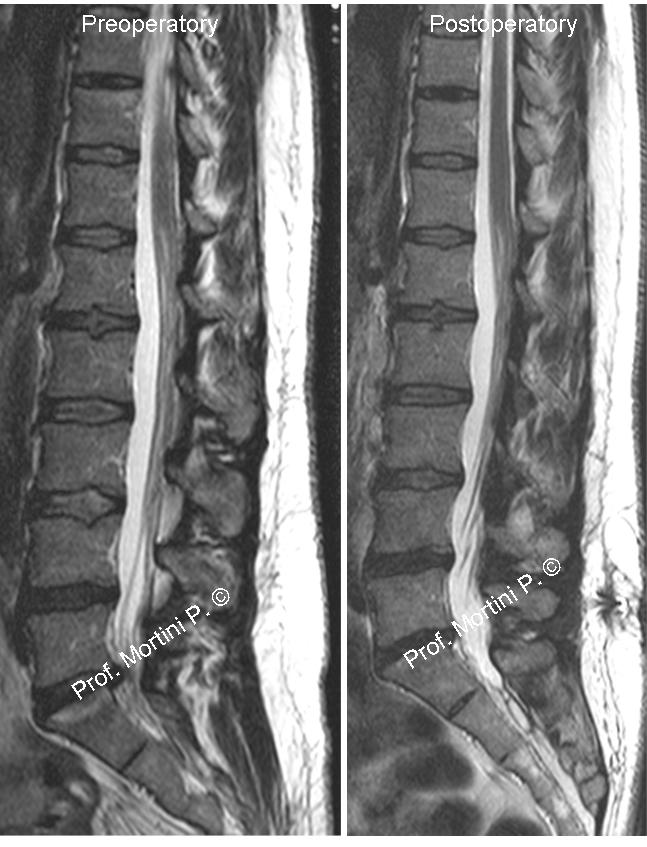
Surgery for patients with disc disorders of the spine is usually reserved for those who have failed exhaustive attempts at conservative treatment over a period of 6-12 weeks.
An incision is placed in the lower back over the area where the disc is herniated. Some bone from the back of the spine is removed to gain access to the area where the disc is located. Typically, the herniated part of the disc and any extra loose pieces of disc are removed from the disc space.
After surgery, restrictions may be placed on the patient’s activities for several weeks while healing is taking place to prevent another disc herniation from occurring. Your physician will discuss any restrictions with you.