English
English Italiano
ItalianoSpinal dysraphism is the term used to refer to developmental abnormalities of the spine. In a normal embryo, the brain and spinal cord develop out of a fold of tissue called the neural tube, which closes completely to form the spinal column.
Failure of the neural tube to close completely results in the birth defect named spina bifida that is the most common form of spinal dysraphism.
In children with spina bifida, there is a gap in backbone and spinal canal, and a portion of the spinal cord and the meninges, the membrane that covers the brain and spinal cord, may protrude out of the back.
The cause of this neural tube defect is not known, but genetics and folate deficiency are thought to play roles. Viral infection, certain medications, and environmental conditions, such as radiation, also may have an effect. Approximately 80 percent of spina bifida cases occur in the lower back.
There are three varieties of spina bifida:
• Spina bifida occulta, the least severe form of the defect, the spinal column does not close, but the meninges and spinal cord do not emerge from the back and skin covers the opening. This is the most common form of spina bifida, but its incidence is unknown because it frequently does not cause symptoms.
• Spina bifida cystica, meningocele defects occur in one of every 1000 births, when part of the meninges protrudes from the back but the spinal cord is normal.
• Spina bifida cystica myelomeningocele is the most severe form of spina bifida is . In children with this condition, a portion of the spinal cord, covered by the meninges, projects from the back. spina bifida myelomeningocele accounts for up to 94 percent of spina bifida cases.
Symptoms
Spina bifida occulta may cause no symptoms at all, but the other forms of the defect usually are serious conditions that can cause a range of neurological problems.
Myelomeningocele causes severe damage to the spinal cord and the nerves that emerge from it at and below the site of the defect. Therefore, symptoms depend on the site of the defect; the higher up on the back the defect occurs, the more problems the child will have.
These effects can include
- paralysis
- loss of sensation in the legs
- loss of bladder and bowel control
Children with myelomeningocele are susceptible to hydrocephalus, a build-up of cerebrospinal fluid around the brain that can cause
- increased head size
- headache
- vomiting
- neurological damage
Syringomelia, another condition that affects children with spina bifida, causes a fluid-filled cavity within the spinal cord, which leads to loss of sensation and motor control.
Spina bifida also can leave children open to a serious infection called meningitis; muscle and bone problems, such as curvatures in the back, hip dislocations, ankle and foot deformities, and contracted muscles; and Chiari malformations, which affect the brainstem and cerebellum and may or may not cause symptoms.
Diagnosis
Before a child is born, blood tests and amniocentesis, a sampling of the fluid that surrounds the embryo, can indicate the presence of neural tube defects.
These tests are not always correct, so ultrasound is used to confirm the diagnosis. Once the baby is born, spina bifida cystica is visible as a sac-like protrusion on the lower back. In children with spina bifida occulta, a tuft of hair or a dimple may indicate the site of the defect. Neurological examination will be conducted to assess the level of impairment.
Further tests to assess the defect after birth include:
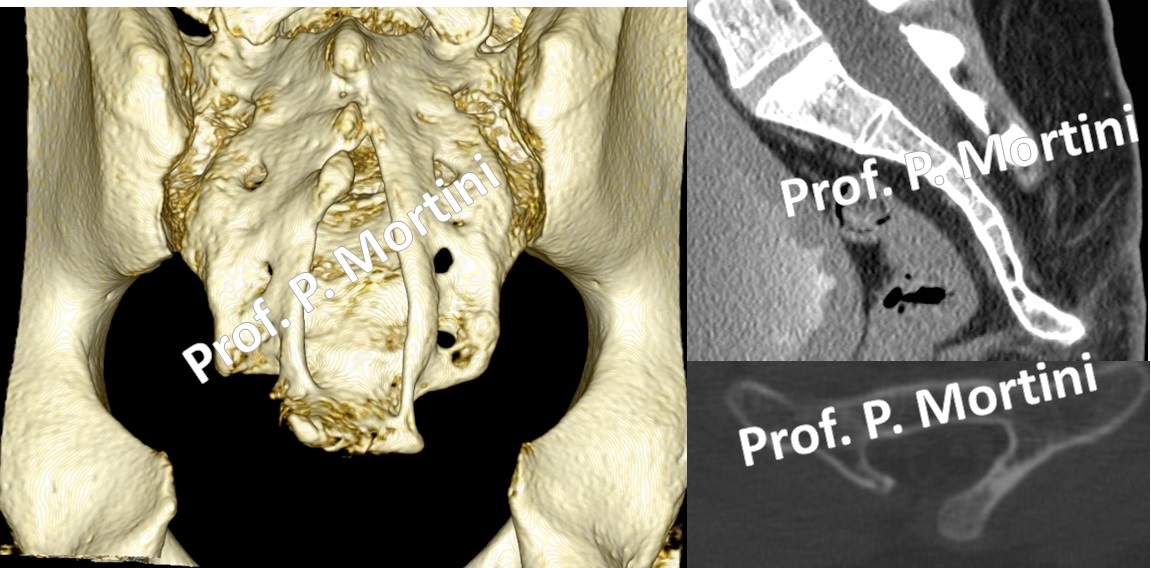
• Spinal x-rays
• Ultrasound
• Magnetic resonance imaging (MRI) scans
• Computed tomography (CT) scans
Treatment
Infants with spina bifida occulta usually do not need treatment. Treatment for the more serious forms of spina bifida requires surgery to correct the defect to limit neurological damage.
Surgery must be conducted as soon as the infant is able to tolerate the procedure, usually within 24 hours of birth. The procedure will restore the proper placement of the meninges and spinal cord and close the opening in the back to prevent infection.
In specialized Centers multi-disciplinary surgical teams may perform surgery to correct neural tube defects or minimize neurological damage before birth.
Because most children with myelomeningocele also have hydrocephalus, treatment may include the implantation of a shunt, a tube that allows the excess cerebrospinal fluid to drain to other parts of the body.
Following the correction of the defect, additional examination and surgery may be required to address orthopedic and urologic problems.
Learning disabilities and developmental delays are common. In addition, long-term rehabilitation often is required after surgery. Babies with spina bifida also are at high risk of developing a latex allergy due to exposure to latex from multiple medical and surgical procedures.